|
|
Welsh Research and Education Network
ARCHIVEAbstracts, articles and publications from completed WREN projects.
|
All Wales Audit into the Management of Respiratory Distress Syndrome (RDS) in Preterm Infants
C Course, M Chakraborty (2015)
Welsh Regional Neonatal Intensive Care Unit, Cardiff, UK
Welsh Regional Neonatal Intensive Care Unit, Cardiff, UK
Aims:
Respiratory Distress Syndrome is the commonest morbidity of preterm infants. We aimed to audit the management of all infants <34 weeks gestational age (GA) born throughout Wales in a 6-month period (between September 2014 to March 2015), against the European Consensus Group guidelines on the Management of RDS published in 2013, to assess our regional practice.
Methods:
Utilising the Welsh Research and Education Network, a proforma was circulated to Welsh neonatal units to prospectively collect data. The proforma encompassed various management strategies covering prenatal care, delivery room stabilisation, surfactant therapy, mechanical and non-invasive ventilation strategies and supportive care.
Results:
Seven units participated (three tertiary units, four level two units) and collected data on 225 infants.
Respiratory Distress Syndrome is the commonest morbidity of preterm infants. We aimed to audit the management of all infants <34 weeks gestational age (GA) born throughout Wales in a 6-month period (between September 2014 to March 2015), against the European Consensus Group guidelines on the Management of RDS published in 2013, to assess our regional practice.
Methods:
Utilising the Welsh Research and Education Network, a proforma was circulated to Welsh neonatal units to prospectively collect data. The proforma encompassed various management strategies covering prenatal care, delivery room stabilisation, surfactant therapy, mechanical and non-invasive ventilation strategies and supportive care.
Results:
Seven units participated (three tertiary units, four level two units) and collected data on 225 infants.
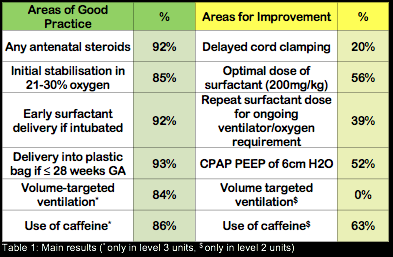
Conclusions:
Areas highlighted for intervention by the audit include promoting the practice of delayed cord clamping on labour ward, the need for education around the dosing of rescue surfactant, the optimal level of PEEP whilst on CPAP and additionally, for level 2 units, the benefits of caffeine therapy. A Welsh Neonatal Network RDS guideline is in discussion and development, with the aim of re-auditing practice across Wales within a year after introduction.
Areas highlighted for intervention by the audit include promoting the practice of delayed cord clamping on labour ward, the need for education around the dosing of rescue surfactant, the optimal level of PEEP whilst on CPAP and additionally, for level 2 units, the benefits of caffeine therapy. A Welsh Neonatal Network RDS guideline is in discussion and development, with the aim of re-auditing practice across Wales within a year after introduction.
Presentations/Publications:
Poster Presentation at British Association of Perinatal Medicine (BAPM) Annual Scientific Meeting 2015, held in Robinson College, Cambridge on 6th November 2015.
Oral Presentation at Welsh Paediatric Society (WPS) Autumn Conference 2015, Held at The Parkway Hotel, Cwmbran on 13th November 2015.
Oral Presentation at the Wales Neonatal Network Annual Audit & Outcome Day on 7th October 2015.
Directly led to the development of the Wales Neonatal Network Guideline for the Management of Respiratory Distress Syndrome in Preterm Infants. Available here.
Poster Presentation at British Association of Perinatal Medicine (BAPM) Annual Scientific Meeting 2015, held in Robinson College, Cambridge on 6th November 2015.
Oral Presentation at Welsh Paediatric Society (WPS) Autumn Conference 2015, Held at The Parkway Hotel, Cwmbran on 13th November 2015.
Oral Presentation at the Wales Neonatal Network Annual Audit & Outcome Day on 7th October 2015.
Directly led to the development of the Wales Neonatal Network Guideline for the Management of Respiratory Distress Syndrome in Preterm Infants. Available here.
Are we using Chest Radiographs Appropriately?
K Greenwood, H Murch, R Hanks
Noah's Ark Children's Hospital for Wales, Cardiff, UK
Noah's Ark Children's Hospital for Wales, Cardiff, UK
Introduction:
Previous studies including Welsh National Audit on management of Broncholitis have stimulated interest to assess appropriateness of CXR requests within Welsh paediatric departments. Basic standards of advice exist for bronchiolitis, viral induced wheeze and community acquired pneumonia. The current usage of CXR’s needs to be explored and appropriateness evaluated.
Aims:
To audit appropriateness of CXR requests in children presenting with bronchiolitis, community acquired pneumonia or viral induced wheeze, against national guidelines.
Methods:
Prospective observational study performed from 13th October to 13th November 2014, across general paediatric departments in Wales. Structured questionnaires completed, with questions based upon: CXR request reasons, clinical diagnosis pre CXR and management plan pre and post CXR.
Results:
9 hospitals participated. A total of 183 cases received, 76 of these were omitted as request reasons were outside the project remit, leaving a total of 107 cases. Table 2 illustrates the reasons for CXR requests. 16% of chest radiographs performed were indicated as per national guidance. Chest radiographs did not alter clinical management in 98% nor alter clinical diagnosis in 100%.
Conclusions:
A unique study involving CXR requests in doctors practising across Wales. This study highlights the overuse of chest radiographs as when used inappropriately do not alter clinical diagnosis or management. This has cost and radiation implications for the paediatric population. We recommend a quality improvement project aiming to decrease numbers of unnecessary CXR’s requested in general paediatric departments across Wales.
Previous studies including Welsh National Audit on management of Broncholitis have stimulated interest to assess appropriateness of CXR requests within Welsh paediatric departments. Basic standards of advice exist for bronchiolitis, viral induced wheeze and community acquired pneumonia. The current usage of CXR’s needs to be explored and appropriateness evaluated.
Aims:
To audit appropriateness of CXR requests in children presenting with bronchiolitis, community acquired pneumonia or viral induced wheeze, against national guidelines.
Methods:
Prospective observational study performed from 13th October to 13th November 2014, across general paediatric departments in Wales. Structured questionnaires completed, with questions based upon: CXR request reasons, clinical diagnosis pre CXR and management plan pre and post CXR.
Results:
9 hospitals participated. A total of 183 cases received, 76 of these were omitted as request reasons were outside the project remit, leaving a total of 107 cases. Table 2 illustrates the reasons for CXR requests. 16% of chest radiographs performed were indicated as per national guidance. Chest radiographs did not alter clinical management in 98% nor alter clinical diagnosis in 100%.
Conclusions:
A unique study involving CXR requests in doctors practising across Wales. This study highlights the overuse of chest radiographs as when used inappropriately do not alter clinical diagnosis or management. This has cost and radiation implications for the paediatric population. We recommend a quality improvement project aiming to decrease numbers of unnecessary CXR’s requested in general paediatric departments across Wales.
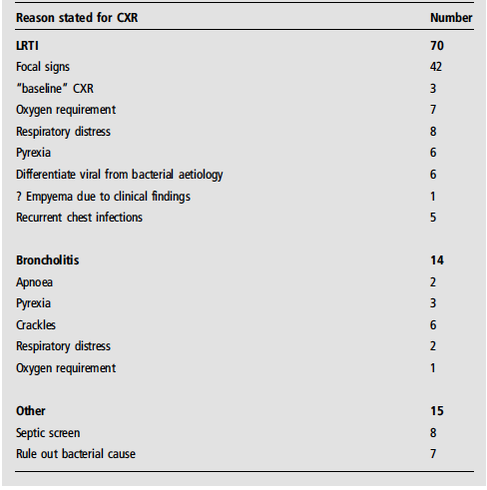
Figure 1: Reasons for requesting a Chest Radiograph
Presentations/Publications:
Oral Presentation at Welsh Paediatric Society (WPS) Autumn Conference 2015, Held at The Parkway Hotel, Cwmbran on 13th November 2015.
Oral Presentation at Royal College of Paediatrics and Child Health Conference 2016.
Published as an abstract in Archives of Disease in Childhood 2016 Vol 101 (supplement 1) pp A186-A187. Available here.
Oral Presentation at Welsh Paediatric Society (WPS) Autumn Conference 2015, Held at The Parkway Hotel, Cwmbran on 13th November 2015.
Oral Presentation at Royal College of Paediatrics and Child Health Conference 2016.
Published as an abstract in Archives of Disease in Childhood 2016 Vol 101 (supplement 1) pp A186-A187. Available here.
UK Survey into the Practices and Beliefs Surrounding Delayed Cord Clamping (DCC)
C Course, M Chakraborty (2016)
Welsh Regional Neonatal Intensive Care Unit, Cardiff, UK
Welsh Regional Neonatal Intensive Care Unit, Cardiff, UK
Aims:
High-quality evidence supports the practice of delayed cord clamping (DCC) for up to 60 seconds in term and preterm infants, reducing the rates of short-term and potential long-term morbidity. An all-Wales audit into the management of respiratory distress syndrome in preterm infants found that the rates of DCC in infants born at <34 weeks gestation was low (20%). We aimed to survey opinion regarding UK healthcare professional’s attitudes and practices around DCC.
Methods:
Using an online platform (SmartSurveyÒ), a twelve question survey was designed, targeting a multi-disciplinary population who undertake care of new-born infants. The first three questions collected demographic data, the next five questions collected data regarding their current practice of DCC, and the last four questions regarding their beliefs around DCC.
The survey was publicised with announcements via the British Association of Perinatal Medicine and Royal College of Paediatrics and Child Health (RCPCH) Regional Offices’ websites and newsletters, and through midwifery contacts at the Royal College of Midwives (RCM). The TwitterÒ platform was used by to attract followers of the RCPCH, RCM and Royal College of Obstetrics and Gynaecology feeds. The survey remained open for six months.
Results:
There were 143 complete responses to the survey (73% midwives, 11% neonatologists, 6% paediatricians, 10% other professionals). 83.2% of responders reported that DCC was practised in their department, but with only 42.7% being aware of a formal departmental guideline for the practice. 88.1% practice DCC in all term infants (³37 weeks gestation), 35.6% practice in preterm infants, and only 6.8% practice in infants <28 week gestation. 89.8% delayed clamping for at least 60 seconds in term infants, however in preterm infants the duration prior to clamping was more varied, with 87.9% believing it should be performed, but 41.4% unsure of how long it was delayed for in their department. 89.5% of responders felt a clinical guideline would aid their practice.
Conclusions:
Despite healthcare professional’s belief that DCC is beneficial there is currently a wide variation of practice, especially in the preterm population. A nationally endorsed guideline would help standardise management in this vulnerable population.
High-quality evidence supports the practice of delayed cord clamping (DCC) for up to 60 seconds in term and preterm infants, reducing the rates of short-term and potential long-term morbidity. An all-Wales audit into the management of respiratory distress syndrome in preterm infants found that the rates of DCC in infants born at <34 weeks gestation was low (20%). We aimed to survey opinion regarding UK healthcare professional’s attitudes and practices around DCC.
Methods:
Using an online platform (SmartSurveyÒ), a twelve question survey was designed, targeting a multi-disciplinary population who undertake care of new-born infants. The first three questions collected demographic data, the next five questions collected data regarding their current practice of DCC, and the last four questions regarding their beliefs around DCC.
The survey was publicised with announcements via the British Association of Perinatal Medicine and Royal College of Paediatrics and Child Health (RCPCH) Regional Offices’ websites and newsletters, and through midwifery contacts at the Royal College of Midwives (RCM). The TwitterÒ platform was used by to attract followers of the RCPCH, RCM and Royal College of Obstetrics and Gynaecology feeds. The survey remained open for six months.
Results:
There were 143 complete responses to the survey (73% midwives, 11% neonatologists, 6% paediatricians, 10% other professionals). 83.2% of responders reported that DCC was practised in their department, but with only 42.7% being aware of a formal departmental guideline for the practice. 88.1% practice DCC in all term infants (³37 weeks gestation), 35.6% practice in preterm infants, and only 6.8% practice in infants <28 week gestation. 89.8% delayed clamping for at least 60 seconds in term infants, however in preterm infants the duration prior to clamping was more varied, with 87.9% believing it should be performed, but 41.4% unsure of how long it was delayed for in their department. 89.5% of responders felt a clinical guideline would aid their practice.
Conclusions:
Despite healthcare professional’s belief that DCC is beneficial there is currently a wide variation of practice, especially in the preterm population. A nationally endorsed guideline would help standardise management in this vulnerable population.
Presentations/Publications:
Poster presentation at British Association of Perinatal Medicine (BAPM) Annual General and Scientific Meeting held in Bristol on 16th September 2016
Poster presentation at British Association of Perinatal Medicine (BAPM) Annual General and Scientific Meeting held in Bristol on 16th September 2016
Indications and Timings of CT Head Scans in Children with Head Injury.
M Atim-Oluk, L Stuttaford
Paediatric Trainees, Wales Deanery
Paediatric Trainees, Wales Deanery
Background:
Head injury is defined as trauma to the head excluding superficial injuries to the face and is responsible for the most frequent cause of death and disability in those aged between 1 and 40 years. Children present to hospital with an estimated annual incidence rate of 400 per 100,000 population. NICE updated their head injury guidelines in January 2014. They use triage tools within their head injury guideline to assist the clinician by providing clinical indications for and timing of T head scans in the department.
Aims:
To audit the indication and timing of CT head scans in head injury in the emergency department (ED) post NICE's updated 2014 guidance throughout Wales.
Methods:
Retrospective and prospective audit across 11 hospitals in Wales over 4 months October-February 2015-2016.
Results:
Data was obtained from 132 CT head scans. Our data consists of 94 males cases (71%) and 25 cases (19%) were aged under one year. CT head sc was indicated within NICE guidance in 87 cases (66%) and performed within an hour in 66 cases (50%). CT head was reported within one hour in 81 cases (61%) though results are unknown in 10 cases (8%).
Conclusions:
In a significant minority of cases we are not following NICE guidance regarding indications for CT head scans in head injury. We need to improve o our time taken to perform CT head scans.
Recommendations:
We recommend dissemination of results across all ED departments in Wales followed by a re-audit in due course.
Head injury is defined as trauma to the head excluding superficial injuries to the face and is responsible for the most frequent cause of death and disability in those aged between 1 and 40 years. Children present to hospital with an estimated annual incidence rate of 400 per 100,000 population. NICE updated their head injury guidelines in January 2014. They use triage tools within their head injury guideline to assist the clinician by providing clinical indications for and timing of T head scans in the department.
Aims:
To audit the indication and timing of CT head scans in head injury in the emergency department (ED) post NICE's updated 2014 guidance throughout Wales.
Methods:
Retrospective and prospective audit across 11 hospitals in Wales over 4 months October-February 2015-2016.
Results:
Data was obtained from 132 CT head scans. Our data consists of 94 males cases (71%) and 25 cases (19%) were aged under one year. CT head sc was indicated within NICE guidance in 87 cases (66%) and performed within an hour in 66 cases (50%). CT head was reported within one hour in 81 cases (61%) though results are unknown in 10 cases (8%).
Conclusions:
In a significant minority of cases we are not following NICE guidance regarding indications for CT head scans in head injury. We need to improve o our time taken to perform CT head scans.
Recommendations:
We recommend dissemination of results across all ED departments in Wales followed by a re-audit in due course.
Presentations/Publications:
Given as an oral presentation at the Welsh Paediatric Society Autumn Conference, held at Miskin Manor, South Wales on 18th November 2016.
Given as an oral presentation at the Welsh Paediatric Society Autumn Conference, held at Miskin Manor, South Wales on 18th November 2016.
A Quality Improvement Project to Meet Training Needs: A Trainee-led Development of a National Multi-Centre Network in Wales
H Murch, C Course, I Morris
Noah's Ark Children's Hospital for Wales, Cardiff, UK
Noah's Ark Children's Hospital for Wales, Cardiff, UK
Introduction:
Paediatric trainees in Wales have raised concerns regarding limited opportunities to become involved in research, audit or quality improvement projects. Smaller ‘in-house’ projects are often described as time-consuming and unfulfilling, are replicated across units, and do not endow trainees with project leadership skills. We aimed to provide a facility to allow high-quality, multi-centre projects to be undertaken more easily across Wales.
Methods:
A focus group of trainees and paediatric and neonatal consultants discussed strategies to overcome these problems. This led to the development of the Welsh Research and Education Network (WREN). This comprises an executive committee, who consider and select project proposals, and regional representatives, who help to co-ordinate selected projects. WREN meetings also contain educational talks on topics relevant topics.
Results:
WREN was founded two years ago and, although still in its infancy, has been highly effective and remains a trainee-led initiative. Two projects have been completed, being presented at both regional and national conferences, and are being submitted for publication. One has led to a new all-Wales guideline being implemented. A further project is nearing completion, with new proposals being invited. Those involved have gained essential skills on leadership of multi-centre projects, alongside fulfilling training requirements, and have produced high-quality work which is influencing patient care across Wales.
Conclusion:
Using a co-operative, co-ordinated approach, it is possible to maximise trainee experience of audit and research, offer leadership and management experience, and can lead to the production of high-quality, clinically relevant work which directly improves patient care.
Paediatric trainees in Wales have raised concerns regarding limited opportunities to become involved in research, audit or quality improvement projects. Smaller ‘in-house’ projects are often described as time-consuming and unfulfilling, are replicated across units, and do not endow trainees with project leadership skills. We aimed to provide a facility to allow high-quality, multi-centre projects to be undertaken more easily across Wales.
Methods:
A focus group of trainees and paediatric and neonatal consultants discussed strategies to overcome these problems. This led to the development of the Welsh Research and Education Network (WREN). This comprises an executive committee, who consider and select project proposals, and regional representatives, who help to co-ordinate selected projects. WREN meetings also contain educational talks on topics relevant topics.
Results:
WREN was founded two years ago and, although still in its infancy, has been highly effective and remains a trainee-led initiative. Two projects have been completed, being presented at both regional and national conferences, and are being submitted for publication. One has led to a new all-Wales guideline being implemented. A further project is nearing completion, with new proposals being invited. Those involved have gained essential skills on leadership of multi-centre projects, alongside fulfilling training requirements, and have produced high-quality work which is influencing patient care across Wales.
Conclusion:
Using a co-operative, co-ordinated approach, it is possible to maximise trainee experience of audit and research, offer leadership and management experience, and can lead to the production of high-quality, clinically relevant work which directly improves patient care.
Presentations/Publications:
Given as an oral presentation at the Welsh Paediatric Society Autumn Conference, held at Miskin Manor, South Wales on 18th November 2016.
Published as an abstract in Archives of Disease in Childhood Vol 101 Supplement 1 pages A319-A320 Available here.
Given as an oral presentation at the Welsh Paediatric Society Autumn Conference, held at Miskin Manor, South Wales on 18th November 2016.
Published as an abstract in Archives of Disease in Childhood Vol 101 Supplement 1 pages A319-A320 Available here.
Auditing referrals to Audiology and Public Health following a diagnosis of meningitis for children within the Cardiff and Vale and Aneurin Bevan Health Boards
F. Astill, S. Lloyd, L. Stuttaford, E. Powell and A. Roberts
Aims
Bacterial meningitis affects around 5 children in every 100,000 each year across the UK and is the commonest cause of acquired hearing impairment in children. Up to 10% of survivors develop sensorineural hearing loss, due to the spread of infection from CSF in the subarchnoid space, via the cochlear aqueduct.
Public Health should be notified of all children with meningitis and children should be referred to and seen by audiology within 4-6 weeks of being well in accordance with NICE guidelines.
Our aim was to identify children that had been referred to, and determine whether they were seen within the recommended timeframe.
Methods
Patient lists were obtained from the audiology and microbiology departments of the health boards and from Public Health Wales. These were amalgated for each health board. We focussed on cases of confirmed meningococcal or pneumococcal disease with a positive blood culture and/or CSF culture or PCR.
Results
Within Cardiff and Vale we confirmed 34 cases of meningococcal disease and 14 cases of pneumococcal disease.
Of the 34 meningococcal cases, 27 children resided within the local area and were eligible for follow-up with audiology with the trust. Only 85% of these children were referred and of those referred 65% were seen within 4-6 weeks of discharge from hospital. The children seen beyond the 6 week time frame were for the majority non-attenders at appointments provided.
Of the 14 pneumococcal cases, 6 children lived within the local area but only 4 of those were referred to audiology. Of those 4, all were seen within 6 weeks.
Within Anuerin Bevan we confirmed 4 cases of each meningococcal and pneumococcal disease. All were referred to audiology and offered an appointment within the recommended timeframe. However there were again a number of non-attenders at appointments.
Of note, of the children who underwent audiological testing none showed signs of hearing impairment.
It became apparent that Public Health had not been notified of all of these cases and this was rectified.
Conclusion and discussion
The number of confirmed cases of meningococcal and pneumococcal disease was higher than anticipated within the Cardiff and Vale health board but this was thought to be due to the presence of Wales’ only PICU within this trust.
The data demonstrates that not all cases were being adequately referred to audiology or Public Health and has suggested a need for re-education of the need for referral and perhaps a more robust system. This is now more pertinent as Public Health Wales have recently changed their stance and will no longer be referred children to audiology themselves, as they previously had as a safety net as it is no longer felt that hearing loss was a public health issue and was an individual one.
Presentations and Awards
British Association of Paediatricians in Audiology Regional Meeting – Cardiff, September 2016
British Association of Paediatricians in Audiology National Meeting – London, January 2017
British Association of Paediatricians in Audiology National Meeting Prize Presentation – London, January 2017
Welsh Research and Education Network Meeting – Bridgend, November 2017
Aims
Bacterial meningitis affects around 5 children in every 100,000 each year across the UK and is the commonest cause of acquired hearing impairment in children. Up to 10% of survivors develop sensorineural hearing loss, due to the spread of infection from CSF in the subarchnoid space, via the cochlear aqueduct.
Public Health should be notified of all children with meningitis and children should be referred to and seen by audiology within 4-6 weeks of being well in accordance with NICE guidelines.
Our aim was to identify children that had been referred to, and determine whether they were seen within the recommended timeframe.
Methods
Patient lists were obtained from the audiology and microbiology departments of the health boards and from Public Health Wales. These were amalgated for each health board. We focussed on cases of confirmed meningococcal or pneumococcal disease with a positive blood culture and/or CSF culture or PCR.
Results
Within Cardiff and Vale we confirmed 34 cases of meningococcal disease and 14 cases of pneumococcal disease.
Of the 34 meningococcal cases, 27 children resided within the local area and were eligible for follow-up with audiology with the trust. Only 85% of these children were referred and of those referred 65% were seen within 4-6 weeks of discharge from hospital. The children seen beyond the 6 week time frame were for the majority non-attenders at appointments provided.
Of the 14 pneumococcal cases, 6 children lived within the local area but only 4 of those were referred to audiology. Of those 4, all were seen within 6 weeks.
Within Anuerin Bevan we confirmed 4 cases of each meningococcal and pneumococcal disease. All were referred to audiology and offered an appointment within the recommended timeframe. However there were again a number of non-attenders at appointments.
Of note, of the children who underwent audiological testing none showed signs of hearing impairment.
It became apparent that Public Health had not been notified of all of these cases and this was rectified.
Conclusion and discussion
The number of confirmed cases of meningococcal and pneumococcal disease was higher than anticipated within the Cardiff and Vale health board but this was thought to be due to the presence of Wales’ only PICU within this trust.
The data demonstrates that not all cases were being adequately referred to audiology or Public Health and has suggested a need for re-education of the need for referral and perhaps a more robust system. This is now more pertinent as Public Health Wales have recently changed their stance and will no longer be referred children to audiology themselves, as they previously had as a safety net as it is no longer felt that hearing loss was a public health issue and was an individual one.
Presentations and Awards
British Association of Paediatricians in Audiology Regional Meeting – Cardiff, September 2016
British Association of Paediatricians in Audiology National Meeting – London, January 2017
British Association of Paediatricians in Audiology National Meeting Prize Presentation – London, January 2017
Welsh Research and Education Network Meeting – Bridgend, November 2017
Delivery of botulinum toxin injection for children with spasticity: a Service Evaluation Project in Pembrokeshire
Dr Nahar Q, Dr Jayasinghe S, Dr Vipulendran V
Department of Child Health, Withybush General Hospital, Haverfordwest
Introduction
Management of spasticity in children should be goal focused and individualised. Evidence suggests botulinum toxin injection is helpful in management of spasticity. In Pembrokeshire, this service is delivered by a network team. Whilst appreciating the specialist and expensive nature of the service, we reviewed the botulinum delivery service in a rural DGH. We measured the standard of care against the NICE guideline.
Method
Retrospective analysis of case notes of all children who received botulinum toxin injection in a single calendar year (2016). A database was created for future analysis.
Results
A total of 39 children were booked in for botulinum toxin injection. All children were reviewed in multidisciplinary clinic prior to the injection. 86% of the patients had their injection within 3 months of the review. The injections were given by paediatricians under local/ general anaesthetic or sedation. There were no reported side effects from the sedation or botulinum toxin injection.
83% children were discharged within 6 hours. 73% patients were reviewed by the team within 6 weeks and different types of therapies were used to improve their function and mobility. Total cost of the injection in 2016 was just over twelve thousand pounds.
Conclusion
The quality and safety of botulinum toxin delivery system is of paramount importance. A dedicated network team of health care professionals should work together to provide an effective service. We have designed an evidence based model to improve the quality and effectiveness of this service and would like to share our model of change.
Presentations
Oral presentation at the Welsh Paediatric Society Autumn Conference 2017 - Saundersfoot November 2017
Poster presentation at the British Paediatric Neurology Association Conference, London 2018
Correspondence
Dr Qumrun Nahar
Withybush General Hospital
email : [email protected], Phone: 01437764545 (ext 3855)
Department of Child Health, Withybush General Hospital, Haverfordwest
Introduction
Management of spasticity in children should be goal focused and individualised. Evidence suggests botulinum toxin injection is helpful in management of spasticity. In Pembrokeshire, this service is delivered by a network team. Whilst appreciating the specialist and expensive nature of the service, we reviewed the botulinum delivery service in a rural DGH. We measured the standard of care against the NICE guideline.
Method
Retrospective analysis of case notes of all children who received botulinum toxin injection in a single calendar year (2016). A database was created for future analysis.
Results
A total of 39 children were booked in for botulinum toxin injection. All children were reviewed in multidisciplinary clinic prior to the injection. 86% of the patients had their injection within 3 months of the review. The injections were given by paediatricians under local/ general anaesthetic or sedation. There were no reported side effects from the sedation or botulinum toxin injection.
83% children were discharged within 6 hours. 73% patients were reviewed by the team within 6 weeks and different types of therapies were used to improve their function and mobility. Total cost of the injection in 2016 was just over twelve thousand pounds.
Conclusion
The quality and safety of botulinum toxin delivery system is of paramount importance. A dedicated network team of health care professionals should work together to provide an effective service. We have designed an evidence based model to improve the quality and effectiveness of this service and would like to share our model of change.
Presentations
Oral presentation at the Welsh Paediatric Society Autumn Conference 2017 - Saundersfoot November 2017
Poster presentation at the British Paediatric Neurology Association Conference, London 2018
Correspondence
Dr Qumrun Nahar
Withybush General Hospital
email : [email protected], Phone: 01437764545 (ext 3855)
Antibiotic Use on the Postnatal Ward: Striking the Balance
Course C1, Greenwood A1, Howard Z2
1Paediatric Trainee, Wales Deanery
2Neonatal GRID Trainee, Wales Deanery
Introduction:
Initiating antibiotic treatment based on risk factors for sepsis is a common practice for newborn infants following publication of the NICE guideline on early-onset neonatal sepsis in 2012. This project aimed to assess the adherence to and impact of this guideline across Welsh units.
Methods:
Utilising the Welsh Research and Education Network (WREN), anonymized data was prospectively collected on infants born in Welsh maternity units starting antibiotic therapy for suspected sepsis across a six-month period. Data on risk factors and clinical indicators of sepsis, demographics, pathology results and management were collected.
Results:
Data on 274 babies from seven units was available for analysis. The mean gestational age was 39+3 weeks. 81.5% started antibiotic treatment for presence of risk factors. 54% had ³2 risk factors. 18.5% had a clinical sepsis indicator. 64.7% of babies were born to mothers being treated for sepsis. 8.4% of mothers were GBS carriers. Only 36% received antibiotics within an hour of treatment decision. 113 infants (41%) had biochemical indicator of sepsis (CRP >9). 2% had positive blood cultures (CONS/“Contaminant”). 30% had a lumbar puncture. All CSF cultures were negative. 11% were admitted to SCBU. Median postnatal ward stay was 3 days, with a total of 995.5 ward days.
Conclusions:
Early-onset neonatal sepsis can carry high morbidity and mortality, which can be exacerbated by delayed treatment. However, the low yield of significant culture results in a cohort that generally were clinically well brings into question the discriminating ability of the risk factors used, and diagnostic tests available, to identify sepsis.
Presented at the Welsh Paediatric Society Spring Conference 2018, International Neonatology Association Congress 2018, Ghent Belgium and Wales Neonatal Network Audit Day 2018
1Paediatric Trainee, Wales Deanery
2Neonatal GRID Trainee, Wales Deanery
Introduction:
Initiating antibiotic treatment based on risk factors for sepsis is a common practice for newborn infants following publication of the NICE guideline on early-onset neonatal sepsis in 2012. This project aimed to assess the adherence to and impact of this guideline across Welsh units.
Methods:
Utilising the Welsh Research and Education Network (WREN), anonymized data was prospectively collected on infants born in Welsh maternity units starting antibiotic therapy for suspected sepsis across a six-month period. Data on risk factors and clinical indicators of sepsis, demographics, pathology results and management were collected.
Results:
Data on 274 babies from seven units was available for analysis. The mean gestational age was 39+3 weeks. 81.5% started antibiotic treatment for presence of risk factors. 54% had ³2 risk factors. 18.5% had a clinical sepsis indicator. 64.7% of babies were born to mothers being treated for sepsis. 8.4% of mothers were GBS carriers. Only 36% received antibiotics within an hour of treatment decision. 113 infants (41%) had biochemical indicator of sepsis (CRP >9). 2% had positive blood cultures (CONS/“Contaminant”). 30% had a lumbar puncture. All CSF cultures were negative. 11% were admitted to SCBU. Median postnatal ward stay was 3 days, with a total of 995.5 ward days.
Conclusions:
Early-onset neonatal sepsis can carry high morbidity and mortality, which can be exacerbated by delayed treatment. However, the low yield of significant culture results in a cohort that generally were clinically well brings into question the discriminating ability of the risk factors used, and diagnostic tests available, to identify sepsis.
Presented at the Welsh Paediatric Society Spring Conference 2018, International Neonatology Association Congress 2018, Ghent Belgium and Wales Neonatal Network Audit Day 2018
UK trainee-led paediatric governance collaboratives: improving the lives of both trainees and children
Helen McDermott1, Hannah Vawda1, Kate Christina Harvey1, Siwan Lloyd2, Christopher William Course2, Rebecca Broomfield2, Annabel Greenwood2, Timothy Mason3, Jeremy Kirk1,4,5
- Paediatric Research Across the Midlands, Health Education West Midlands, Birmingham, UK
- WREN, Wales Deanery, UK
- PenTRAIN, Health Education South West, Bristol, UK
- Clinical Research Network, NIHR Clinical Director, West Midlands, UK
- Consultant Endocrinologist, Birmingham Children’s Hospital, Birmingham, UK
Abstract: Research is vital to paediatrics; however, many trainees feel there is a deficit in their opportunities, experience and exposure in this area. Three training regions in the UK, the West Midlands, Wales and Peninsula, have recently started region-wide, trainee-led research and governance collaboratives aimed at improving trainee access and education in research, undertaking good quality, multicentre audit, quality improvement and pilot projects in collaboration across the regions and implementing change. We report on the experiences, benefits and challenges of these trainee collaboratives (Paediatric Research Across the Midlands, Wales Research and Education Network and Peninsula Trainee Research Audit and Innovation Network) including a trainee survey looking at how these initiatives have improved skills in conducting multicentre prospective studies, team working skills, leadership, understanding of statistics and manuscripts and presentation skills. We also describe how collaboration with colleagues and participation in projects can benefit trainees in a wider sense of purpose and help to encourage morale, as well as what can be learnt as paediatric training moves forward.
Published in Archives of Disease in Childhood: Education & Practice
McDermott H, Vawda H, Harvey KC, et al
UK trainee-led paediatric governance collaboratives: improving the lives of both trainees and children
Archives of Disease in Childhood - Education and Practice Published Online First: 09 May 2019. doi:10.1136/archdischild-2018-316354
Available at: https://ep.bmj.com/content/early/2019/05/09/archdischild-2018-316354
McDermott H, Vawda H, Harvey KC, et al
UK trainee-led paediatric governance collaboratives: improving the lives of both trainees and children
Archives of Disease in Childhood - Education and Practice Published Online First: 09 May 2019. doi:10.1136/archdischild-2018-316354
Available at: https://ep.bmj.com/content/early/2019/05/09/archdischild-2018-316354
The Management of Respiratory Distress Syndrome in Preterm Infants: The Changing Experience in Wales
Christopher Course(1,2), Mallinath Chakraborty(1,3)
(1)Welsh Regional Neonatal Intensive Care Unit, Cardiff, UK. (2)Neonatal Registrar, Wales Deanery, UK. (3)Cardiff University, Cardiff, UK
(1)Welsh Regional Neonatal Intensive Care Unit, Cardiff, UK. (2)Neonatal Registrar, Wales Deanery, UK. (3)Cardiff University, Cardiff, UK
Background
Respiratory Distress Syndrome (RDS) is the commonest diagnosis after premature birth, a result of structural and functional immaturity of the lungs. These preterm infants often require invasive and non-invasive respiratory support, supplementary oxygen and surfactant therapy. A proportion of these infants will go on to develop chronic lung disease of prematurity, with abnormal respiratory function and increased respiratory morbidity persisting through childhood and into adult life. There exists a wealth of high-quality evidence on optimal management of RDS. We aimed to describe trends in management before and after introduction of a national guideline in Wales on RDS management.
Methods
Anonymised, prospective data from all participating neonatal units (level two and level three) in Wales were collected in two six-month time periods in 2015 and 2018 for all inborn infants <34 weeks’ gestation using a standardised proforma. A national guideline for management of RDS in preterm infants was introduced in 2016 by the Wales Neonatal Network. Data collection included areas of antenatal management, delivery room stabilisation, invasive and non-invasive respiratory support, surfactant treatment and elements of supportive care. Univariate and multivariate methods were used to compare data between the two epochs. Odds ratios and 95% confidence intervals (CI) were adjusted for gestational age at delivery and level of unit of delivery. Statistical significance was set at p < 0.05.
Results
Data on 225 infants from 2015 and 276 infants in 2018 was analysed. Mean gestational age and birthweight were comparable between the epochs (p > 0.05). Comparing care before and after introduction of the guideline, there was overall improvement in use of targeted tidal volume ventilation (aOR 7.94 [3.75,16.8]), caffeine therapy (aOR 2.49 [1.4,4.6]), oxygen therapy post-surfactant (aOR 2.16 [1.23,3.82]) and early use of parenteral nutrition (aOR 2.75 [1.66,4.58]). Areas of poorer management included use of high positive end expiratory pressures (aOR 0.58 [0.35,0.96]) and stabilisation in FiO2 <30% (aOR 0.29 [0.17,0.47]). Little variation was seen between level two and three units, although more mature infants had significantly higher rates of delayed cord clamping (DCC) (aOR 1.44 [1.23,1.68]), stabilisation on CPAP (aOR 1.85 [1.65,2.07]), and early enteral feeding (aOR 1.22 [1.12,1.32]).
Conclusions
We present novel data from Wales collected around the implementation of a new national RDS guideline. Significant improvements in management of RDS in preterm infants were seen, particularly regarding mechanical ventilation. Yet some practices such as DCC, struggle to be embraced. Despite large volumes of high-quality evidence, some elements of best practice are yet to be adopted consistently. Further work should focus on education and training.
Respiratory Distress Syndrome (RDS) is the commonest diagnosis after premature birth, a result of structural and functional immaturity of the lungs. These preterm infants often require invasive and non-invasive respiratory support, supplementary oxygen and surfactant therapy. A proportion of these infants will go on to develop chronic lung disease of prematurity, with abnormal respiratory function and increased respiratory morbidity persisting through childhood and into adult life. There exists a wealth of high-quality evidence on optimal management of RDS. We aimed to describe trends in management before and after introduction of a national guideline in Wales on RDS management.
Methods
Anonymised, prospective data from all participating neonatal units (level two and level three) in Wales were collected in two six-month time periods in 2015 and 2018 for all inborn infants <34 weeks’ gestation using a standardised proforma. A national guideline for management of RDS in preterm infants was introduced in 2016 by the Wales Neonatal Network. Data collection included areas of antenatal management, delivery room stabilisation, invasive and non-invasive respiratory support, surfactant treatment and elements of supportive care. Univariate and multivariate methods were used to compare data between the two epochs. Odds ratios and 95% confidence intervals (CI) were adjusted for gestational age at delivery and level of unit of delivery. Statistical significance was set at p < 0.05.
Results
Data on 225 infants from 2015 and 276 infants in 2018 was analysed. Mean gestational age and birthweight were comparable between the epochs (p > 0.05). Comparing care before and after introduction of the guideline, there was overall improvement in use of targeted tidal volume ventilation (aOR 7.94 [3.75,16.8]), caffeine therapy (aOR 2.49 [1.4,4.6]), oxygen therapy post-surfactant (aOR 2.16 [1.23,3.82]) and early use of parenteral nutrition (aOR 2.75 [1.66,4.58]). Areas of poorer management included use of high positive end expiratory pressures (aOR 0.58 [0.35,0.96]) and stabilisation in FiO2 <30% (aOR 0.29 [0.17,0.47]). Little variation was seen between level two and three units, although more mature infants had significantly higher rates of delayed cord clamping (DCC) (aOR 1.44 [1.23,1.68]), stabilisation on CPAP (aOR 1.85 [1.65,2.07]), and early enteral feeding (aOR 1.22 [1.12,1.32]).
Conclusions
We present novel data from Wales collected around the implementation of a new national RDS guideline. Significant improvements in management of RDS in preterm infants were seen, particularly regarding mechanical ventilation. Yet some practices such as DCC, struggle to be embraced. Despite large volumes of high-quality evidence, some elements of best practice are yet to be adopted consistently. Further work should focus on education and training.
Poster display and presentation at the 3rd Congress of joint European Neonatal Societies (jENS), Maastricht, the Netherlands, 14th-21st September 2019
Oral Presentation at Welsh Paediatric Society Autumn Conference, 8th November 2019
Publication: Course, C., & Chakraborty, M. (2020). Management of Respiratory Distress Syndrome in Preterm Infants In Wales: A Full Audit Cycle of a Quality Improvement Project. Scientific reports, 10(1), 3536. https://doi.org/10.1038/s41598-020-60091-6
Oral Presentation at Welsh Paediatric Society Autumn Conference, 8th November 2019
Publication: Course, C., & Chakraborty, M. (2020). Management of Respiratory Distress Syndrome in Preterm Infants In Wales: A Full Audit Cycle of a Quality Improvement Project. Scientific reports, 10(1), 3536. https://doi.org/10.1038/s41598-020-60091-6
Changes in the Management of Respiratory Distress Syndrome in Welsh Preterm Infants – seven years’ experience
Celyn Kenny,1,3, Mallinath Chakraborty1,3, Christopher Course2,3
1Welsh Regional Neonatal Intensive Care Unit, Cardiff, UK. 2Neonatal Grid Trainee, Health Education and Improvement Wales, UK. 3Cardiff University, Cardiff, UK
Introduction:
Respiratory Distress Syndrome (RDS) is common following preterm birth, often requiring respiratory support, supplemental oxygen, and exogenous surfactant. We describe RDS management in Welsh-born preterm infants since 2015.
Methods:
Anonymised, prospective data collected from Welsh neonatal units (level two and three) during three six-month periods (2015, 2018 and 2021) for inborn infants <34 weeks’ gestation, during implementation of a national guideline (2016, updated 2019). Data collected included antenatal and delivery room management, invasive and non-invasive respiratory support, surfactant treatment and supportive care. Statistical analysis included univariate and multivariate regression, with odds ratios (OR) adjusted for gestational age and unit level of delivery.
Results:
Data from 766 infants was collected across three epochs, with comparable gestational ages and birthweights (p>0.05). Comparing care between epochs, antenatal steroid exposure remained high with marked improvements in the practice of delayed cord clamping (OR 4.24; 95%CI 3.22,5.58) and early oxygen management (1.45; 1.14,1.84). Significant improvements were noted in volume targeted ventilation use (4.14; 2.66,6.47), optimal surfactant dosing (1.60; 1.17,2.18) and surfactant administration via less invasive methods (InSurE) (2.19; 1.29,3.69). Enteral feeding within the first day of life significantly improved (2.04; 1.67,2.48). There was a non-significant trend towards increase in stabilisation with non-invasive support at birth (1.20; 0.94,1.53), and delivery into a plastic bag for infants born <28 weeks gestation (77% in 2015, 86% in 2021, p=0.23).
Conclusions:
We demonstrated multiple improvements in RDS management since 2015. Further work should focus on encouraging thermoregulation and non-invasive respiratory support at birth and optimising early parenteral nutrition.
Celyn Kenny,1,3, Mallinath Chakraborty1,3, Christopher Course2,3
1Welsh Regional Neonatal Intensive Care Unit, Cardiff, UK. 2Neonatal Grid Trainee, Health Education and Improvement Wales, UK. 3Cardiff University, Cardiff, UK
Introduction:
Respiratory Distress Syndrome (RDS) is common following preterm birth, often requiring respiratory support, supplemental oxygen, and exogenous surfactant. We describe RDS management in Welsh-born preterm infants since 2015.
Methods:
Anonymised, prospective data collected from Welsh neonatal units (level two and three) during three six-month periods (2015, 2018 and 2021) for inborn infants <34 weeks’ gestation, during implementation of a national guideline (2016, updated 2019). Data collected included antenatal and delivery room management, invasive and non-invasive respiratory support, surfactant treatment and supportive care. Statistical analysis included univariate and multivariate regression, with odds ratios (OR) adjusted for gestational age and unit level of delivery.
Results:
Data from 766 infants was collected across three epochs, with comparable gestational ages and birthweights (p>0.05). Comparing care between epochs, antenatal steroid exposure remained high with marked improvements in the practice of delayed cord clamping (OR 4.24; 95%CI 3.22,5.58) and early oxygen management (1.45; 1.14,1.84). Significant improvements were noted in volume targeted ventilation use (4.14; 2.66,6.47), optimal surfactant dosing (1.60; 1.17,2.18) and surfactant administration via less invasive methods (InSurE) (2.19; 1.29,3.69). Enteral feeding within the first day of life significantly improved (2.04; 1.67,2.48). There was a non-significant trend towards increase in stabilisation with non-invasive support at birth (1.20; 0.94,1.53), and delivery into a plastic bag for infants born <28 weeks gestation (77% in 2015, 86% in 2021, p=0.23).
Conclusions:
We demonstrated multiple improvements in RDS management since 2015. Further work should focus on encouraging thermoregulation and non-invasive respiratory support at birth and optimising early parenteral nutrition.